October 2, 2018
Work Programs Should Help, Not Harm, Virginia Families: Thousands Likely to Lose Coverage under Waiver
This report was updated to reflect the most current information, as of October 2018. Original report was released in July 2018.
In June 2018, Governor Northam signed a budget that included Medicaid expansion, a policy that was estimated to provide health coverage to nearly 400,000 low-income individuals throughout the state. The legislation creates a dual-track approach to expansion — one is to expand Medicaid coverage under the rules of the Affordable Care Act, and the other is to apply to the Centers for Medicare and Medicaid Services (CMS) for a waiver to take Medicaid coverage away from many people who aren’t working or engaged in work-related activities. In September 2018, the state released the text of the proposed waiver, which will go through a 30 day state comment period, followed by a 60 day federal comment period, and then will be sent to CMS for approval.
All evidence suggests that work requirements as written in the proposed waiver will be burdensome for all involved — individuals and families as well as the state — and will lead to more than 21,000 people losing health coverage. As policymakers proceed, they should look to available evidence to make informed decisions about how to structure a new program effectively.
This issue brief highlights concerns which decision makers should take into account as they move forward with this process. It also outlines proven policy solutions for improving employment outcomes for low-income individuals and families — including ways Virginia’s proposed work requirement program can be shaped to mitigate some likely negative impacts.
Demonstration Waivers and Work Requirements
The adopted budget provides the state’s Medicaid office, the Department of Medical Assistance Services (DMAS), with the authority to amend the state’s Medicaid plan to provide Medicaid health coverage to adults who earn less than 138 percent of the poverty level ($16,753 for a single person or $28,676 for a family of three in 2018). It also directs DMAS to submit to CMS the 1115 waiver application. Of the 32 other states that have already expanded Medicaid, only a handful have done so through a waiver. Virginia is the only state to attempt a dual-track approach — where the state is working to expand Medicaid coverage and also apply for a waiver to impose work requirements at the same time.
Waivers, like the one proposed by Virginia, are supposed to allow states to take an innovative approach to furthering the objectives of the Medicaid program. CMS suggests that such approaches would include improving access to care and promoting program efficiency. These waivers must also support the mission of Medicaid, which is to provide care to people “whose income and resources are insufficient to meet the costs of necessary medical services.” It is through this waiver, in addition to other stipulations, that the state of Virginia seeks to impose work requirements on those enrolled in the Medicaid program. (Notably, the first state to be approved for work requirements, Kentucky, has already lost a lawsuit on the grounds that its waiver will not support the mission of Medicaid.)
Specifically, the 2018-2020 enacted budget establishes the Training, Education, Employment, and Opportunity Program (TEEOP). The language included in the final budget outlining TEEOP is largely based on HB338, which was passed by the House and left in the Senate during the 2018 legislative session. The fiscal impact statement attached to that bill during its consideration in the session provides important insights into the costs of standing up a new work program. With some exceptions, TEEOP requires Medicaid enrollees between the ages of 18 and 64 to eventually work or volunteer at least 80 hours every month. The requirements include a suspension provision, meaning that if enrollees miss that target for any three months out of a twelve month period, they will lose health coverage. Suspended enrollees may be able to enroll again if they are able to demonstrate certain compliance behaviors.

According to fiscal analysis of HB338, the amount of funding allocated in the final budget would only be enough to enforce compliance with the work requirements — a low intervention approach. There is not adequate funding to provide assistance for low-income individuals to find a job and people would simply lose health coverage if they were unable to keep up with the paperwork or could not work at least 80 hours per month. This is despite budget language saying the program “shall include career services for program enrollees, services to link enrollees with industry certification and credentialing programs, including the New Economy Workforce Credential Grant Program, and individualized case management services.” The waiver makes clear that many of these “supports may be contingent on the appropriation of additional State funding by the State Legislature.” If lawmakers are serious about these goals, then they should be ready to allocate appropriate funding.
Health Coverage Supports Work
The ability of a state to impose work requirements on Medicaid enrollees is new, as it was not until January 2018 that any state was allowed to take this action. At the beginning of September 2018, Arkansas became the first state to remove low-income people from their Medicaid coverage for not meeting work requirements (4,353 people were removed from the program out of 26,000 people subject to the requirements).
Efforts to take away public supports for the purpose of “promoting” work have been attempted before in other social support programs across the country over the past several decades and have poor track records. Work requirements have failed to boost long-term employment or improve general welfare. In many cases, these proposals have made it harder for individuals to find work, which hurts their family members, including children.
The mere existence of burdensome work reporting requirements may also deter families from enrolling in public coverage for which they qualify. When someone does not have health coverage, they are less able to seek medical care for their needs and are in turn generally less able to secure work. When surveyed, the vast majority of people who are newly covered under Medicaid expansion in other states cite the new coverage as making it easier to look for, secure, or maintain employment. While the goal of TEEOP is “to enable enrollees to increase their health and well-being through community engagement leading to self-sufficiency,” the specifics of the program are likely to become barriers to health care and to work itself.
A Costly Program for a Small Group of People

A work requirement program in Virginia will be expensive, and it’s important to note that the vast majority of Medicaid enrollees are already working, disabled, ill, caretakers, pregnant women, students, retired, or looking for work. Only around 1 percent of enrollees don’t fit into one of those categories, according to national data. This means that the state would incur additional expenses and administrative work to enforce a requirement that the vast majority of people are complying with already or unable to.
Pulling the Rug Out in Times of Most Need
The nature of the jobs that many low-income Virginians work make it doubly challenging to meet the proposed work requirement threshold of 80 hours a month. The two most common occupations for adults in Virginia who could qualify for Medicaid under expansion are food services (9.7 percent) and construction (5.9 percent). Both of these occupations can be seasonal and are prone to irregular hours. That means that while a worker may have more than a full-time load of work one month, they may fall below the 80-hour threshold the next month and could be subject to losing their health coverage.
During the past recession, unemployment in Virginia soared, like much of the country, and few companies were hiring. Virginia’s existing Medicaid program was available to help parents who lost their job and therefore their health insurance, even if they could not find new work. Medicaid work requirements would make the situation much worse for struggling families across the commonwealth. Just when an individual or family might need Medicaid coverage the most during a downturn in the job market, unless an individual is able to find employment with at least 80 hours of work a month in a short time frame, then they may not be able to keep Medicaid coverage.
Worse, regional disparities in job markets could exacerbate problems finding a job. When we look at average unemployment rates over the past 5 years in Virginia, rural areas of the state, particularly Southwest and Southside, have struggled the most. That means that while an individual may want to meet work requirement standards, if they live in a locality with a relatively high unemployment rate, then they are going to have more trouble doing so. According to the budget language, if an individual lives in an area where the unemployment rate is 150 percent of the state average, then they can be exempt from having to find employment. If “areas” ends up meaning localities, Virginians living in many counties and cities close to this threshold are out of luck for getting the employment exemption. Someone living on one side of a county line could have access to coverage, while their neighbor in the same work and life situation living just over the line would be left out.
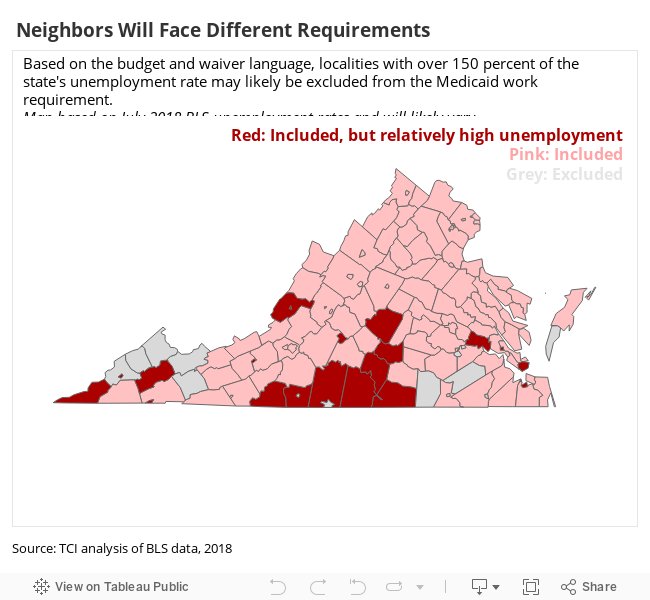
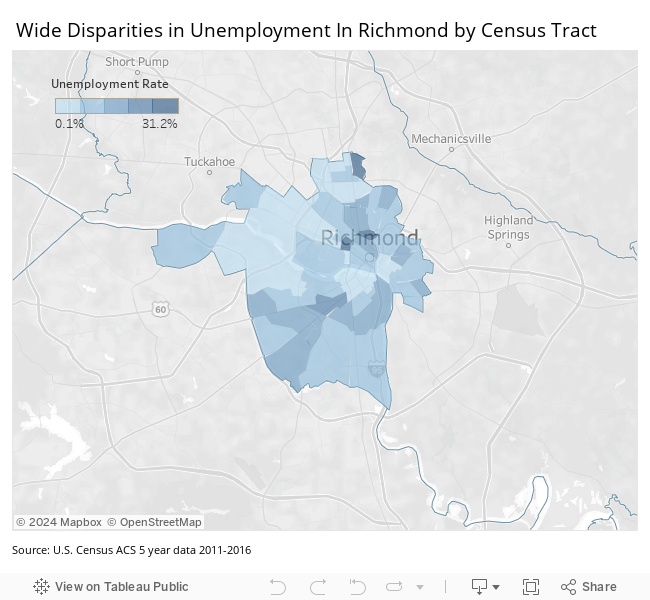
And many localities that will not be exempt have major disparities in employment. For example, in Richmond (the locality with the second highest income disparity in the state), many parts of the city have higher unemployment rates than any locality in the state. However, because more well-off areas of the city — likely parts that would not benefit as much from Medicaid expansion — bring the overall unemployment levels down, struggling parts of the city are still not exempt. This problem is present in localities throughout the state, but is exaggerated in cities.
As surveys in other states have shown, having consistent health insurance would likely bolster job search efforts during times of underemployment and unemployment.
Working People Likely to Be Harmed By a Work Requirement
Even if someone does find a job or meet other requirements for Medicaid, the increased paperwork and reporting that would come with work requirements in Virginia would likely lead to a share of individuals losing coverage due to the challenges — for enrollees and administrators — of navigating a complicated system. Some studies have shown that nearly one third of SNAP recipients (formally known as food stamps) who lost coverage due to work requirements had conditions that should have been identified and made them exempt. Other studies consistently show that individuals who are removed from Temporary Assistance for Needy Families (TANF) benefits for not meeting work requirements are more likely to have a disability compared to those who continue to receive benefits. These disabilities, which would exempt individuals from work requirements, are often not identified by the service providers in charge of enforcement.
Additional barriers to work will exist for many struggling Virginians that will likely not be exempt by the provisions of TEEOP. For example, in Arkansas, the first state to actually enact work requirements for Medicaid, an estimated 78 percent of the individuals who will be subject to the work requirements and don’t currently work either have no vehicle, no internet access at home, less than a high school education, have a serious health issue, or are caring for someone with a serious health issue. Any of these barriers may not exempt a person under Virginia’s current work requirement language, but Virginia policymakers should work to structure any program in such a way as to effectively deal with these very real barriers low-income workers face.
Read more: Work Requirements are Uniquely Challenging for Those with Mental Health Needs
Barriers Lead to Losses
The stated purpose of 1115 waivers — in part, to improve access and promote program efficiency — is not consistent with the likely results of a work requirement in Virginia. Additional reporting and administrative work, lack of support services, and suspension provisions will lead to people losing health care. In Kentucky, the first state to be approved by CMS to tie work requirements to Medicaid, nearly a quarter of new enrollees from their state’s expansion population would lose coverage as a result of this change over the next 5 years (nearly 100,000 people). That’s because Kentucky — like Virginia — planned to include in the new monthly work requirements some caretakers, retired individuals, part-time students, ill and disabled people who have not been deemed “medically frail,” those already looking for work, and part-time workers not working 80 hours per month.
Virginia’s work requirements will mainly apply to newly eligible Medicaid enrollees. The Virginia Department of Medical Assistance Services estimates that at least 21,600 low-income adults could be removed from Medicaid under the proposed work requirements.
Costly And Ineffective
The budget estimates show the state cost of starting work requirements will be more than $25 million. This is partially due to the lack of supportive services, and also likely includes the loss in expected Medicaid savings from thousands of low-income individuals being kicked off from coverage as a result of these new requirements. This means it will cost the state additional money to kick people off of Medicaid because these individuals will still seek medical services, and the state will end up picking up some of that expense without the federal match rate to assist with those costs.
Without funding for adequate work support or sufficient exemptions for those unable to work, the current work requirement language is leading the state down a path that will not improve employment, will kick people off their coverage, and will ultimately cost the state more money. It’s not too late for Virginia to change course by focusing on not removing people from their health coverage and using the savings and other funds to invest in support that actually leads to long-term employment.
Alternative Approaches for Boosting Employment
While the current funding and plan for Medicaid work requirements is not likely to improve employment and well-being among low-income Virginians, there are a few time-tested policies that have a track record of improving employment.
Research shows that over time, punitive work requirement programs can often backfire, while programs focused on training individuals for decent jobs are effective at boosting long-term employment. Looking at a collection of work requirement schemes across the country, the Center on Budget and Policy Priorities found that some work requirement programs were associated with a modest increase or decrease in employment in the first two years, but in later years, the effects were mostly negligible to negative.
In the same review, there were two work support programs that were actually found to be effective in boosting employment — one in Portland, Oregon and one in Riverside, California. Both of these programs offered intensive education, training, and job search support for all recipients until they were gainfully employed. What made these programs even more unique though, was that each one encouraged individuals to not take low-paying jobs and to hold out for better options. Five years after the start of these work requirement programs, individuals who received support services were 6 to 13 percent more likely to be employed than those who did not go through the program.
New Hampshire has had a program where unemployed Medicaid enrollees are referred to the state-run job search program rather than being subjected to punitive measures if they fail to find a job themselves, although this may change as new work requirements are enacted in the state. Voluntary work support programs, like the one that has existed in New Hampshire, can be highly effective and a large majority of unemployed individuals, 3 out of 4, choose to participate in these programs at well-implemented sites when given the opportunity.
Similarly, Montana has implemented a successful work promotion program that identifies barriers Medicaid enrollees have in joining the workforce and works with them to build skills, connect them to training, and find long-term employment. The program has had a high participation rate, largely credited to the extensive outreach campaign that the state undertook.
Virginia is currently not considering any program that would be this intensive for supporting finding well-paying work. Even the high touch approach that was outlined in HB338, estimated to cost $178 million for state and local governments over the first two years, would still fall far short of this degree of support. Consequently, the version of work requirements devised at this point in Virginia will at best lead to negligible change in employment for low-income individuals over the long term, at worst, it could very well reduce employment for these individuals.
Read more: TANF Work Requirements: A Cautionary Case Study in Virginia
Moving Forward
The goal of TEEOP is “to enable enrollees to increase their health and well-being through community engagement leading to self-sufficiency.” As Virginia moves forward with the waiver application process for work requirements, policymakers should seek to build on best practices from other states, and include a comprehensive evaluation of the Virginia program to learn its impact. Given how politicized work requirements are in Virginia, the evaluation should be done by a neutral party, such as a university, to determine if the waiver is actually improving health outcomes, as is required by CMS guidelines.
Policymakers should also consider strengthening the likelihood of success by providing adequate funding for work training and increasing long-term employment. While there is a strong consensus in research on work requirements that they do not fulfil their purported purpose of increasing employment, and that they will in all likely scenarios lead to worse health outcomes, these impacts can be somewhat mitigated by effective work supports. As the state moves forward with this public experiment, policymakers have a responsibility to build on best practices, closely document the outcomes, and be prepared to change course.
Read more from this report:
Work Requirements are Uniquely Challenging for Those with Mental Health Needs


